
Trochlear nerve
The trochlear nerve arises from the trochlear nucleus of the brain, emerging from the posterior aspect of the midbrain (it is the only cranial nerve to exit from the posterior midbrain).
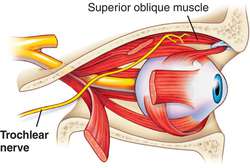
It runs anteriorly and inferiorly within the subarachnoid space before piercing the dura mater adjacent to the posterior clinoid process of the sphenoid bone. The nerve then moves along the lateral wall of the cavernous sinus (along with the oculomotor nerve, the abducens nerve, the ophthalmic and maxillary branches of the trigeminal nerve and the internal carotid artery) before entering the orbit of the eye via the superior orbital fissure.
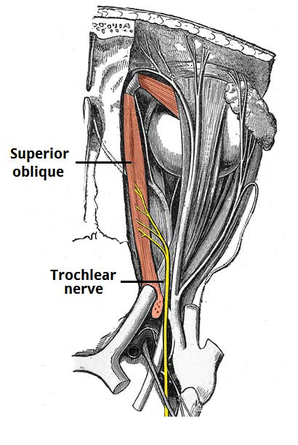
The trochlear nerve innervates a single muscle – the superior oblique, which is a muscle of oculomotion. As the fibres from the trochlear nucleus cross in the midbrain before they exit, the trochlear neurones innervate the contralateral superior oblique.
The tendon of the superior oblique is tethered by a fibrous structure known as the trochlea, giving the nerve its name. Although the mechanism of action of the superior oblique is complex, in clinical practice it is sufficient to understand that the overall action of the superior oblique is to depress and intort the eyeball.
Clinical relevance
Trochlear nerve palsy commonly presents with vertical diplopia, exacerbated when looking downwards and inwards (such as when reading or walking down the stairs). Patients can also develop a head tilt away from the affected side.
They are commonly caused by microvascular damage from diabetes mellitus or hypertensive disease. Other causes include congenital malformation, thrombophlebitis of the cavernous sinus, and raised intracranial pressure.